 Correo Electrónico
Correo Electrónico
 DNINFOA - SIA
DNINFOA - SIA
 Bibliotecas
Bibliotecas
 Convocatorias
Convocatorias
 Identidad UNAL
Identidad UNAL




Diseases caused by infections or parasites make part of the list of forgotten, neglected diseases, according to the classification made by the Pan American Health Organization (PAHO). The interest for developing and improving clinic and pharmaceutical research is limited, and innovation in efficient and economical diagnosis methods is little. These diseases are characterized by the low investment for their control and management.
For the World Health Organization (WHO), the importance of neglected diseases (ND) is their impact and persistence in poor or marginal populations. They are also concerned about their secondary effects in the improvement of health conditions of those who are not attended on time, using safe and efficient therapeutic tools.
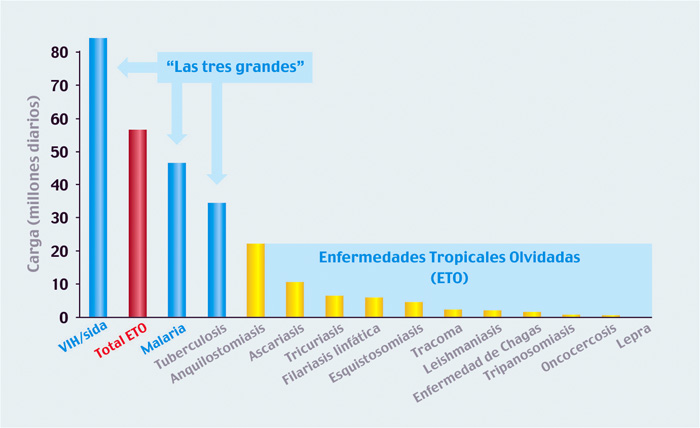
According to the WHO, close to 1,000 million people in the world suffer from one of these diseases (ND). Estimations, compared to those of HIV/AIDS, malaria and tuberculosis, classify them as an important problem in the world (Figure 1).
Leprosy, leptospirosis, the plague, trachoma, Buruli"s ulcer, Chagas, African trypanosomiasis, cutaneous and visceral leishmaniasis, onchocerciasis, dengue, human rabies, dracunculiasis, distomatosis, cholera, schistosomiasis, lymphatic filariasis, geohelmintiasis and ophidian accidents are included in the group of ND made by the WHO
Local scenario
One of the difficulties to determine the situation in Colombia is that just some Neglected Diseases need to be reported immediately, such as human rabies, ophidian accidents, congenital syphilis, cholera, dengue, leishmaniasis, diphtheria, anthrax, those transmitted by food, Chagas, the plague and leprosy.
From this list, those with the highest incidence are dengue (which locates Colombia in the third place in Latin America with the highest number of cases), rabies exposition and leishmaniasis. Estimations for 2010 calculate approximately close to 18 million cases of intestinal parasitosis and 22,000 cases of leishmaniasis.
The country has the conditions that permit the presence of these diseases that occur in populations with low socioeconomic status, high levels of illiteracy, precarious households, overcrowding, and inadequate health services (especially drinking water), in addition to problems in the access to services of public health.
According to the last census made by DANE in 2005, 27.7% of Colombian population has close to 100%, Unsatisfied Basic Needs (UBN) in remote areas far from big urban centers where all the elements are present for ND to persist. Likewise, in 2008, 46% of Colombians were living below the poverty line and 17.8% were homeless.
However, this is not the only risk factor. It is necessary to question the scope of heath programs, in which ethnic minorities (natives and African descendants) children and women are the most affected. The accumulation of all this epidemiologic and social conditions creates a vicious circle.
It is also important to mention that there are deeper differences in the health systems such as the attention models of subsidiary and contributive regime, complementary programs and prepaid health.
Stigmas
All this problems represent long term consequences, as the cases of elephantiasis and filariasis. Some diseases, during the chronic stage, have manifestations with considerable economic costs for the patient and the health systems. Besides, these diseases affect societies, diminishing productivity and the welfare and development of those affected by the disease.
The world has become interested in discussing this topic within the context of the compliance of human rights. In Colombia, the ministry of Social Protection issued Resolution 412 of 2000, which included some of these pathologies. Its actualization in 2006 allowed including others such as American trypanosomiasis or Chagas" disease.
In 2009, the PAHO, of which Colombian is a member, approved resolution Elimination of neglected niseases and other infections related to poorness. It was accepted that their reduction or elimination is possible with the available instruments. For this reason, Member States have undertaken to reduce them until they are not considering a public problem by 2015.
For achieving this objective, the need to improve the surveillance system for diseases in the country was proposed, along with the allocation of efficient resources to achieve the sustainability of control programs based on prevention, diagnosis, treatment, control and elimination strategies. Besides, the creation of "safer accessible diagnosis tests, safer medicines and appropriate mechanisms to reduce late complications was propose."
The most affected countries will be those with higher index of Unsatisfied Basic Needs (UBN) and limited health systems to face the control and implementation of operative programs, with faster diagnosis methods and safe and cheap medicine that permit universal access to affected populations.
The efforts made by the researchers, the academy and some nongovernmental organizations have led to the inclusion of all these disease in the international sanitary agenda, which is evident in a biggest investment, the development of safer medicine and faster and cheaper diagnosis tests for remote areas with difficult access, or politically unstable zones.
Maria Victoria Valero,
PhD in Tropical Medicine and Public Health
Leader of the Complexity and Poorness Group
Universidad Nacional de Colombia